



The disease is unsanctioned behaviour; social distancing: the thin ice under UK Government
It looks very much like UK Government is scrambling to maintain significant levels of respect for its lockdown measures as real world capability of “Covid-19” continues to fail to live up to modelled expectations. As we have already discovered here at FBEL, lockdown is not about controlling disease, but controlling behaviour, and today Boris Johnson reappeared from his supposed convalescence to recast UK Government policy so that it could try and get ahead of the juggernaut of public scorn, disinterest, and indeed tendency to rebellion.
Johnson spoke of the first peak having been passed, but pointed forward towards a new one. The second peak, which according to the official story must happen as the virus seeks out infection of the herd, will require the sustaining of measures “to suppress the disease and keep the reproduction down”. After that, said Johnson, there would be gradual refinement of the “the economic and social restrictions”. He went on:
In that process, difficult judgements will be made. And we simply cannot spell out now how fast or slow or even when those changes will be made, though clearly, the government will be saying much more about this in the coming days.
There have been plenty of clues about what we should presume to see, all coming in the shape of expectation management from corporate-media. Social distancing looks like it is going to be the mitigation measure that is going to stay for as long as the UK Government can make it stick. This makes sense, because while police have no powers to stop anyone being outside, and legislation to prevent assembly would surely end in violence that the UK Government might be able to deal with, but surely wouldn’t want, there can be legislation to alter the way that businesses permit personnel and public to operate on their premises. The talk in corporate-media, accompanied by images of people queuing up outside supermarkets, is that it will become the “new normal” – and if it drives small business to the wall because they cannot accommodate the legislation, then this is par for the course for corporate-government.
Obviously, something must be done to completely overthrow the mass delusion which would empower UK Government to act (and then to deal similarly with UK Government – but one thing at a time). At FBEL, self-empowerment of individuals is a permanent theme, and has been discussed in relation to “Covid-19” through the medium of analysis of the so-called Coronavirus Restriction Regulations, and the eminently pertinent film, Equals. Additionally, a demonstration of what would be normal behaviour, but which is now considered disruptive, has been supplied. More is to follow.
Of equal importance as the promotion of the confidence of the individual in terms of being a power is the continued education regarding the deception that is “Covid-19” and the UK Government’s response to it. Obviously, this is crucial for creating the sense of being aggrieved, and creating motivation for becoming empowered.
As such, in this article we will explore how it is that the Imperial College London (ICL) statistical modellers who gave the UK Government pretext for a lockdown clearly signalled that social distancing was one of the first things that could be terminated when a first peak was considered dealt with†. It is hoped that the reader will see that on this issue, the UK Government has not only moved the goalposts, but attached wheels to them.
To accomplish our purpose, it becomes necessary to have a very good look at what was proposed by the ICL modellers in terms of conditions, not only for locking down, but also ceasing the mitigation measures by various degrees. These conditions were stated in a 16th March publication produced by the “Imperial College COVID-19 Response Team” (emphasis added):
The model reproduces the intervention effect sizes seen in epidemiological studies and in empirical surveys of contact patterns. Two of the interventions (case isolation and voluntary home quarantine) are triggered by the onset of symptoms and are implemented the next day. The other four NPIs [non-pharmaceutical interventions] (social distancing of those over 70 years, social distancing of the entire population, stopping mass gatherings and closure of schools and universities) are decisions made at the government level. For these interventions we therefore consider surveillance triggers based on testing of patients in critical care (intensive care units, ICUs). We focus on such cases as testing is most complete for the most severely ill patients. When examining mitigation strategies, we assume policies are in force for 3 months, other than social distancing of those over the age of 70 which is assumed to remain in place for one month longer. Suppression strategies are assumed to be in place for 5 months or longer.
The reader might notice that home quarantine was supposed to be for people who display symptoms, and was supposed to be voluntary, so the core of the so called lockdown is an overreach by UK Government (if one considers it to be anything other than an invitation to comply). As for the four NPIs that are UK Government options, note that the modellers assume that they terminate. If the UK Government says it is being led by science to maintain social distancing, then this isn’t coming from the models that engendered the lockdown. And by the way, where duration of social distancing is assumed, this appears, in fact, to be related to when certain triggers activate to determine when it can end. The bottom line is that implementation of social distancing is dependent on critical care bed occupancy:
Social distancing and school/university closure are triggered at a national level when weekly numbers of new COVID-19 cases diagnosed in ICUs exceed the thresholds listed under “On trigger” [which is a range of numbers] and are suspended when weekly ICU cases drop to 25% of that trigger value. Other policies are assumed to start in late March and remain in place. The right panel shows the proportion of time after policy start that social distancing is in place.
This text refers to a table that appears (in its right panel) to show the percentage of time when social distancing would be in place in relation to the entire duration when wider mitigation policies are in force (hopefully, if this is not clear, it will become so by example in due course).
As we have gathered, then, at the crux of the issue is the rate of occupancy of critical care unit beds, and as it happens the most recent Intensive Care National Audit & Research (ICNARC) report makes for interesting reading where that is concerned. For the first time it involves a graph showing the daily breakdown for patients in intensive care. This data is all important, and the concept can never be under repeated: lockdown is designed to ease pressure on the NHS, and critical care bed occupancy is the indicator of this pressure.

The ICNARC data tells us that a 400 bed per week take-up looks (from the graph, above) to have been reached in the week up to March 22nd. It also suggests that occupancy rate is declining to levels that would justify the corresponding off-trigger to end social distancing – and that might even happen this current week.
This is problematic because the relevant cell in the right panel of the table mentioned above informs that for a reproduction number of 2.4 (which is what the ICL team has assumed is the value of Rₒ [and for a full explanation, see previous FBEL articles]), with an on-trigger of 400 beds per week, social distancing would be in place for 71% of the time that the full measures remain in place; this seems to tell us that social distancing would have been expected to be necessary for 71% of 5 months, according to the ICL assumption in relation to full suppression. This amounts to, roughly, 3 and a half months.
Obviously, if this all means that the off-trigger is supposed to occur at 3 and a half months (roughly) past the peak, we are in the real world perhaps two and a half months early.
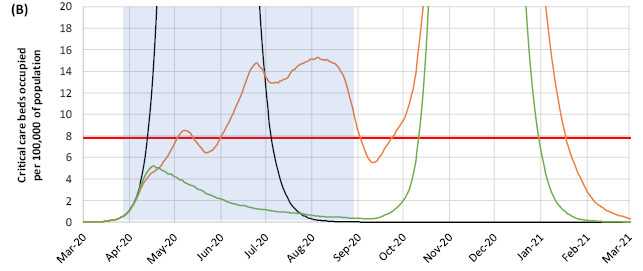
Moreover, if one looks at the predicted path for critical care bed take-up (below [the green line]), after the peak, it is supposed to fall by 4 occupied bed(s) per 100,000 of population (to abbreviate, obp100k) in about 3 months. So, if we now use the new and actual peak date, which looks in terms of critical care bed occupancy to have occurred by the 5th April, reaching the level of 1 bed occupied per 100,000 of population – which represents 625 beds – is something that would occur at the start of July. And this is before we consider how, when the peak happened, critical care bed occupancy was lower than was predicted by 1 obp100k (which is a conservative estimation by the author – working not shown). So this would mean that occupancy would be verging to zero at the start of July.
In fact, the ICNARC data suggests critical care bed take-up falling symmetrically to the way it increased, and we might see the matter resolved (i.e. virtually no occupancy) well before the end of May – or, well before one month after the peak. If social distancing is in place even at that time, surely it would be very difficult indeed to justify. And no, the second peak has not been forgotten of. Instead, it is discarded, because if the first peak was so entirely badly predicted, the second cannot be trusted to manifest as the modelling insists. And ultimately, it is not the point, which is this: perhaps by the end of May, and definitely by the end of June, social distancing, to millions of members of the public, will indubitably appear to be the prison treatment that it is no doubt intended to be.
† As always, the caveat: this is after an assumption that the modelling could have been correct in the first place, and after an assumption that all supposed real time cases of “Covid-19” had anything to do with SARS-COV/SARS-COV-2, and after an assumption that the PCR test to detect the presence of SARS-COV/SARS-COV-2 works.
Further reading:
A coronavirus peak nears (ahead of time), the modelling is clearly wrong, and lockdown unjustified (link)
The smaller, earlier peak; and the determined effort to maintain the lockdown regardless (link)














