



Covid-19: utterly false perception of great danger created by letting some old and ill people die
While one or two articles are due on the topic of a possible link between prescription drugs for high blood pressure and related conditions, and levels of ACE2 in a body, with the intuitive assumption being made that more ACE2 presents greater capacity for binding to it by SARS-COV at the lung, and therefore is perhaps the most important causative element of Covid-19, it does rather amount to discussion of the minute details of a rare illness. That being said, it is crucial for exposing the coronahoax – so there’s no wonder that this piece will come full circle back to the issue even without really touching on it in the journey – and so the promised material will certainly get written.
However, what is required in the world as more of a priority is a piece that very clearly gets to heart of the matter, and thus here it is, presented under a title that summarises everything people need to know about “Covid-19”.
The big fat lie of “Covid-19” is apparent more than ever before because of a disparity between steady and even increasing case numbers (people who have tested positive for “Covid-19” – at least as far as the official definition goes) and the falling off of deaths attributed to the disease.
It shouldn’t be a surprise to see that this disproving phenomenon isn’t being exploited as it should be by alternative media, where simple extrapolation enhanced by application of other knowledge reveals a story of the NHS essentially withdrawing treatment, or death pathway management as it is called here, so that tens of thousands of people died all in one short space of time (instead of over a longer duration) in order that it looked as though these people had been struck down by a virulent disease. This is one part of the story. Through simple ledger entries, people who were going to die imminently had the stigma of “Covid-19” attached to them, sometimes to the great puzzlement of relatives, and the medical practitioners could get away with this because UK Government had prepared the ground for the abuse – as was discussed in the FBEL article, Building the “coronahoax” charge sheet: reckoning culpability for the deliberate inflation of Covid-19 death. Even before the publication of that piece, right at the start of the episode it was recorded in these pages that hospitals were testing, or perhaps more likely making unwarranted clinical diagnoses, on their ICU wards: “Government is casting around amongst the immunosuppressed vulnerable to find indicators of Covid-19 so as to boost figures”.
There were other people in hospitals who, if they could be moved, were expelled and sent to care homes, irrespective (it appears) of whether or not they had been diagnosed as having “Covid-19” (as far as the official definition goes). The full weight of this scandal is still something that has yet to ignite the sort of furore that it should, but even so, as things stand it is a known fact that the NHS did turn out tens of thousands of people to make room for “Covid-19” cases out of the general population. They were cases that never came (so in fact, empty hospitals during the height of the deaths and the disparity between deaths and cases are both a reflection of the same thing: the general population has never been at threat from Covid-19).
By July 3rd, which is the date of a BBC article that reports the figure, 20,000 people were official Covid-19 victims in care homes:
Almost 30,000 more care home residents in England and Wales died during the coronavirus outbreak than during the same period in 2019, ONS figures show.
But only two-thirds were directly attributable to Covid-19.
The bell curve of death had pretty much petered out by the time that the extract first appeared in its original form, so it is safe to say that something approaching 50% of the official death toll took place in care homes. Later, the Daily Mail would announce that “[A] new study reports that 40 per cent of those who died from coronavirus over the first 16 weeks were care home residents.”
The same Mail piece (of August 30th) reports 20,000 dead too, but is sneaky because it quite evidently wants to give the impression that the deaths came from the original residents:
More than 500,000 adults lived in a residential or nursing home at the start or the pandemic and one in 25 is believed to have died from the virus.
Later on in the article, there is the yielding of the centrally important detail that “25,000 patients [were sent] into care homes without tests”.
As mentioned, there have also been hospital deaths, with the Health Service Journal (HSJ) reporting on 9th July that, at that time, the cumulative total was 28,951 in England. While we can take a good bet that all of the care home deaths were palliative in that they involved death by another terminal illness that had nevertheless been attributed to “Covid-19”, in hospitals some of the deaths would have been cases where real mechanics of Covid-19 were involved. These most certainly would have required treatment in an intensive care unit, and the distinction between cases of this sort, and cases where the patient was in palliative care on general wards, is something that was understood very early in at FBEL. The following is an extract from an April article:
The latest Intensive Care National Audit & Research Centre (ICNARC) audit of patients with “Covid-19” in intensive, or critical care in England, Wales and Northern Ireland, reports that only 1499 people have died of the disease in a context of escalated levels of treatment applied to patients suffering with it. To repeat that which has been explained hereabouts before…, the discrepancy with the official number for “Covid-19” deaths in hospitals, which runs into the tens of thousands, and is 10 times larger than that which has occurred in the vast majority of the UK’s intensive care wards, is due to the fact that most people die on general wards. Logic would dictate (because these patients do not die in critical care) that this happens because their treatment has not been curative, but inevitably palliative. And this helps us understand that these people are not necessarily dying of “Covid-19” after all.
As for the actual number of people dead from Covid-19, of which the ICNARC audit figures might be the best indicator, we will arrive at this in due course. But as for the grossly inflated official death toll figure which really has nothing to do with real Covid-19, what we are looking at is a number representing the ending of lives of those who would have died, if not sooner, then certainly later – but hurried up to it with the withdrawal of death pathway management. It was a massacre.
Even if this is an outrage that alternative media can be relied on not to expose, it nevertheless requires covering up. So, very recently (25th August) the Financial Times (FT), in a free to read piece, published a number of talking points that could be used to be seen to explain why people suddenly stopped dying of “Covid-19” in big numbers.
The first excuse offered is that there has been an increased amount of testing, so this is inevitably finding more cases where the subject of the test is not likely to die. Now, the first thing to say about this is that it rides roughshod over claims made at the beginning of the episode by even the very highest in authority that…
None of us are superhuman and impervious to getting sick during this process… And that’s what makes this whole thing so awful for all of us.
This is what Rishi Sunak said using Boris Johnson’s faked illness as the model for his warning. Apparently, such is the UK Government’s faith in the stupidity of the public that unfulfilled promises of the indiscriminate nature of Covid-19 do not present a deterrence from later inventing a rationalisation involving more risk to certain demographics than others. There is no reconciling the “more likely to die”, from the following extract (from the FT), with the previous concept of “everyone at risk”, which now should clearly be understood as having been an outright lie to induce fear at the start of the episode:
“As the epidemic has progressed, tests have become far more widely available,” said Paul Hunter, professor of medicine at the University of East Anglia. “Back in March and April we were mainly testing people who were really ill and more likely to die. Now the programme is catching a much higher proportion of infections with mild or no symptoms.”
The extract betrays that there is a huge overlap from the first into the second excuse that the FT presents in its article, which is this: there has been a change in the age profile of infections. The two issues are so interconnected that one cannot help but deal with them at the same time. However, we’re going to see (as is always maintained at FBEL) that age has nothing to do with the ability to be infected, or indeed dying. It is, instead, a matter of health terrain.
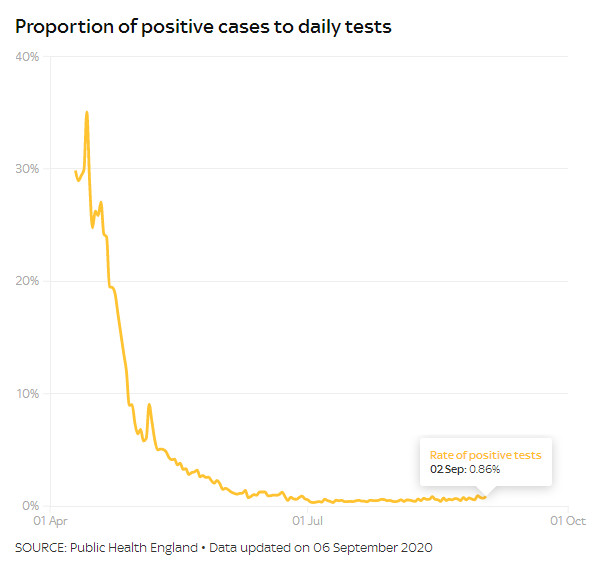 For the time being, it needs to be pointed out that there is no reason to believe the UK Government in anything it says about testing or cases, because no one is holding it to account independently, and the impression of increased testing and cases suits its agenda so that there can be continuation of measures that suggest a threat from a disease. That being said, the cupboard is naturally bare for UK Government of the ingredients needed to drive its hoax, for it appears that the proportion of tests that prove positive is less than 1% – a paltry figure – and has been the case since June. This is a figure that can be got from an otherwise deceptive Sky News article which suggests that case rates are at the highest level since early summer – which they may be, but the difference is a mere matter of tenths.
For the time being, it needs to be pointed out that there is no reason to believe the UK Government in anything it says about testing or cases, because no one is holding it to account independently, and the impression of increased testing and cases suits its agenda so that there can be continuation of measures that suggest a threat from a disease. That being said, the cupboard is naturally bare for UK Government of the ingredients needed to drive its hoax, for it appears that the proportion of tests that prove positive is less than 1% – a paltry figure – and has been the case since June. This is a figure that can be got from an otherwise deceptive Sky News article which suggests that case rates are at the highest level since early summer – which they may be, but the difference is a mere matter of tenths.
Then of course, another problem on the horizon for UK Government is news coming out of the US that as much as 90% of positive PCR tests do not indicate infection with SARS-COV-2 and therefore (potentially putting a crimper on track and trace schemes) do not indicate contagion. Indeed, it is quite possible that the excuse of “more tests” for the death/case disparity is really one that implicates flawed tests (with full disclosure to come) to explain why people are not dying.
The issue is not a new one, and it has cropped up before at FBEL. The PCR test essentially amplifies a sample to detect the virus. In real simple terms, more amplification means increased likelihood of finding a trace of the target. Success in these terms does not indicate infection, because infection requires a good deal of the pathogen – a great good deal of it, in fact. Mere presence of a virus is not the same as infection with a virus.
The Mail carried the story on 30th August; it had first appeared in the New York Times and concerned the implications of a study executed in Massachusetts, New York and Nevada in July (neatly omitting the fact that the PCR test is flawed in exactly the same way in the UK):
Health experts say PCR testing – the most widely used diagnostic test for COVID-19 in the US – are too sensitive and need to be adjusted to rule out people who have insignificant amounts of the virus in their systems because they’re likely not contagious.
This would constitute more data to consider as we, at FBEL, continue to ask the question if there ever can be an asymptomatic case of Covid-19, with ramifications about the question of whether it is possible to be a “super carrier” or “super spreader”. The answer continues to look negative – and new advice from the US Centres for Disease Control are quite entirely devastating (from the Mail):
Last Monday the CDC changed its guidelines, which now say that if you were exposed but don’t have symptoms, ‘you do not necessarily need a test unless you are a vulnerable individual’ or a doctor advises it.
The truth is increasingly becoming plain: the reason why people are not contagious when they are asymptomatically a positive Covid-19 case is because they aren’t actually infected: they don’t have Covid-19‡. Moreover, if there is no infection, there won’t be death. As has been observed at FBEL before, it appears to be the case that there is a neat split where health terrain creates susceptibility to Covid-19 (meaning, where there would be an infection), or it does not. The vast majority will not be host to an infection; they won’t see any development of SARS-COV into a disease.
Indeed, the findings that 90% of people who produce a positive PCR test will not develop Covid-19 can be applied to the official UK death toll figure so that the real numbers of Covid-19 death can be understood. In April, FBEL tracked daily death announcements to find that 95% of people who died of “Covid-19” had comorbidities (for which, read pre-existing conditions) – and it was reasoned that it would be these other illnesses that would be the cause of death. ICNARC, which collates information from hospitals in England, Wales and Northern Ireland, in the last† weekly report it produced, reckoned that accumulatively there had been some 4400 Covid-19 deaths in ICUs (and in after care). All the data does point to real Covid-19 deaths being a figure between 5 and 10% of the official death toll.
This brings us to the next excuse offered by the Financial Times article, which is that improved medical care has meant lower deaths. But this is abject, irrelevant nonsense, because the number of people being admitted to hospital for Covid-19 has fallen to an all time low, as the FT article itself tells:
Rather, hospital admissions and deaths attributed to Covid-19 are at record lows in Britain and several other European countries. In the week ending August 21, British hospitals admitted an average of just over 84 people a day with Covid-19 — less than at any stage during the pandemic.
Three other minor reasons are offered in the Financial Times piece, and the first of these is a possibility that “people are becoming infected with lower ‘viral loads’ now that transmission is taking place mainly in the community rather than in care homes and hospitals”. As the reasoning goes, a “lower dose” of SARS-COV-2 reduces the chance of serious illness.
However, if there is lower rates of infection than thought – as we are officially finding out – then contagion becomes a redundant issue. Moreover, if 90% of “viral loads” in care homes and hospitals did not constitute infection, then there has never been an issue with how much virus is in an environment.
If, though, we accept for a moment that the viral loads idea is a plausible hypothesis, it is something that can’t be demonstrated because the PCR doesn’t measure quantity of virus. It is more plausible to say that the more an immune system in weakened, the more likely an infection will take place, but that opens up a kettle of fish that doesn’t suit the narrative.
The second minor excuse is that deaths are subject to a seasonal influence, so that in summer “people are generally healthier” and conditions not so conducive for survival of the virus outside of a body. Naturally, it begs the question, what’s the connection between the season and how any supposed infection doesn’t develop into Covid-19? Is it that people are generally unwell, and this facilitates deterioration? If so, this is like an explanation along the lines of comorbidities being supplementary to a SARS-COV-2 infection so that death occurs – but as we have seen, in faux-Covid-19 it is the illness that kills, and the virus is irrelevant (assuming it is even present). Ultimately, however, this idea appears not to take into account that the British weather was glorious all the while people were dying of “Covid-19” in March, April and May, so it’s not quite clear where the empirical evidence for the idea comes from.
The third of the minor theories is that the virus is mutating so that it becomes less virulent; this is based on the concept that contagion is a self-defeating aspect of viral evolution. If it is an idea that appears to be counter intuitive, then there is no time to get into a debate about germ theory (instead, see here). However, if we give it credence, how do we know when the virus stopped being infectious and contagious if, actually, 90% of those who were said to have died of it by July in fact died of a comorbidity?
As such, and as abovementioned, the issue of contagion is looking increasingly to be a redundant one. And the reader must understand, it is entirely unclear if the lack of virility now apparently observed in the virus is because of the impact of any herd immune system defence. It could well be that the virus was always a busted flush.
This brings us to the subject of SARS-COV-2 in fact merely being some long distant variation of SARS-COV, or indeed the same thing; it’s an idea that has been posited before in these pages, and works in conjunction with the idea that some other change to the health terrain activates a part of a host’s microbiome that would otherwise be dormant. We do have a confirmed suspect as the agent of the change, even if we’re not exactly sure why: the protein ACE2.
Follow up: Covid-19 in a nutshell (link)
† Update, 9th September
The report in question was the one issued in the last week of July. After that, despite regular checking at the ICNARC site, the author was not able to discover another audit report, and gained the impression that they were no longer being produced. However, a new audit report has now been found at the ICNARC site, dated 7th September, indicating that production never ceased. It will feature in an upcoming article.
‡ Update, 11th December
A thread on Twitter by Michael Yeadon, ex-Pfizer head of respiratory research, date of publication as update:
Those who found the concept of asymptomatic transmission suspect were right to be. Not saying it never happens. Am saying it’s implausible. Here’s why. To transmit, you need to have cultured virus in your airways. And you need to make respiratory manoeuvres sufficient to expel…
…plenty of infected secretions. Here’s the thing. Unless you’re symptomatic, you won’t cough repeatedly. And unless you’ve got plenty of virus in your secretions, it’d be unlikely you will infect someone. But if you’ve grown an infectious culture in your airways, you WILL be…
…symptomatic. This is because either the virus is attacking your tissues & this will make you feel unwell, or because your immune system is fighting the virus, and that, too, makes you feel ill. It’s just implausible to pretend that lots of people somehow harbour intense…
…infection yet have no symptoms. Equally, expulsion of virus doesn’t happen in quantity in exhaled air during tidal breathing. And by definition, violent respiratory actions like coughing, which does, is a symptom. It sounded invented the 1st time I heard it. And it was.














