



A tale of two Covid-19s; potentially, the only real thing is the fight too far picked by UK Government
The latest Intensive Care National Audit & Research Centre (ICNARC) audit of patients with “Covid-19” in intensive, or critical care in England, Wales and Northern Ireland, reports that only 1499 people have died of the disease in a context of escalated levels of treatment applied to patients suffering with it. To repeat that which has been explained hereabouts before (links provided below), the discrepancy with the official number for “Covid-19” deaths in hospitals, which runs into the tens of thousands, and is 10 times larger than that which has occurred in the vast majority of the UK’s intensive care wards, is due to the fact that most people die on general wards. Logic would dictate (because these patients do not die in critical care) that this happens because their treatment has not been curative, but inevitably palliative. And this helps us understand that these people are not necessarily dying of Covid-19 after all.
At the crux of the issue is the difference between the real illness, and other varied ailment which is falsely being attributed to the disease. The former is a pneumonia, and its complications, and the latter is a host of other things corralled under the same umbrella term, “Covid-19”, because of the coincidental presence of the SARS-COV/SARS-COV-2 coronavirus as detected by a PCR test, but sometimes merely by clinical diagnosis after a patient presents certain symptoms. Already, then, we can perhaps see why real Covid-19 would be something to battle against in intensive care, and why “Covid-19” is something that the old and the very ill would succumb to in general wards.
In exploring this difference further, we will commence in the realm of the false disease.
There has been a lot of discussion recently about statistics released by the Office for National Statistics for the week ending the 3rd April. These show that there were 6,082 more deaths in that week than the five-year average. It is claimed by promoters of the official narrative that 3475 deaths that have been attributed to “Covid-19” demonstrate that the disease has caused excess deaths, or unexpected deaths: ones that would not have happened without “Covid-19” as a cause.
We should note that the number reported dead by the ICNARC between 27th March and 3rd April was 261, and by this we can suppose that the vast majority of the ONS’ “Covid-19” death toll comprised of what we might call false cases. This would mean that most of the 6,082 excess deaths, by far and away the vast majority, were not due to Covid-19 – and one would then need to ask, if they really where unexpected, what abnormal phenomenon had caused them?
This requires some breaking down. When one digs into the ONS data, one discovers that 69% of the deaths attributed to “Covid-19” occur to people over the age of 75, and an astonishing 87% occur to people who are older than 65 years of age. Moreover, tracking performed here at FBEL of announcements by NHS England since April 1st has found that only 5% of people whose hospitalised deaths are attributed to “Covid-19” do not have a pre-existing or underlying health issue. In other words, 95% of deaths involve a co-morbidity.
This is hard evidence that most of the 3475 deaths by “Covid-19” reported by the ONS will be false cases, and that the actual number of deaths by April 3rd that realistically could be attributed to Covid-19 would be more in line with the ICNARC figure of 261 (indeed, the FBEL tracking suggests that 253 people in the UK had died of Covid-19 by April 3rd).
Of course, there is a counter argument that says existence of pre-existing illness is irrelevant, because the Covid-19 is the element that finishes people off. But the people who would make dispute in this way are asked to pay attention. Covid-19 (when it kills) is pneumonia, aspects of pneumonia, and pneumonic complications. People who die because they have been overcome by their cancer, for instance, have not died of Covid-19 just because they have been found to be host to the SARS-COV/SARS-COV-2 coronavirus. This is because the PCR test that detects this entity does not, and cannot diagnose an infection. Moreover, if the test returns a positive result, there are good reasons other than the SARS-COV/SARS-COV-2 coronavirus that it would do that: the test is unreliable. The reader is asked to read the FBEL article, Letting flu do the dirty work: the vast potential to misrepresent death as due to Covid-19, which contains a fuller explanation.
So, ultimately the common factor in patients who are old and ill who are said to have died of “Covid-19” is not a coronavirus that cannot be proved to be present, and cannot be proved to have reproduced so as to infect the host. Instead, the common factor, as logic must dictate, is that the patients are old and ill, and had a tendency to die because of those issues.
Now, the next thing to be done to field the objections of a counter-argument is to answer this question: why would doctors in hospitals who sign off death certificates with cause as “Covid-19” lie if it was clear to them that a patient had succumbed to another illness (or old age) and that a coronavirus was coincidental at, or incidental to the death? Any reader who requires an answer needs to follow the same link published immediately above to discover that the UK Government has made changes to the requirements of coroner’s examinations, by the exempting of “Covid-19” from a certain standard of scrutiny, so that abuse and laxity in the “coal-face” filtering on hospital wards is invited. Moreover, the NHS, with guidelines that ultimately mean that a doctor needs no proof of “Covid-19” to diagnose it, has created an environment for this abuse and laxity to occur (see the FBEL article, Coronavirus/Covid-19: the anatomy of a hoax). As such, well meaning medical professionals will usually not understand that there should be doubt about a diagnosis of “Covid-19”, will usually conform to peer pressure, and see no deterrence (because of the exempted status of Covid-19 at the coroner’s stage of examination) to imprecisely attribute a cause of death even if they happened to be conflicted about doing it.
Returning to the phenomenon of excess deaths in the week ending April 3rd, if we saw more people unexpectedly dying of pneumonia, we could call it an indicator of excess mortality that could be attributed to Covid-19. Indeed, while the 5 year average for death by influenza and flu for the week ending April 3rd was 2064, the number that had died by that cause was 2367 – not a very convincing excess amount. As it is, then, we have 6,082 more overall deaths than the average, some of which we might call proper Covid-19, but most attributable to other causes.
And if they are excess death, we certainly can’t call them unexpected, for it appears to be the case that the NHS has created a situation where it has prioritised Covid-19 to such an extent that its usual service has suffered – and examples of how this has been done is explained in the FBEL article, The smaller, earlier peak; and the determined effort to maintain the lockdown regardless. If the denial of service, which took the form of discharging patients already in hospital, stopping treatment for certain non-Covid-19 illness, and having vulnerable people consent negatively to resuscitation protocol, was a deliberate decision, which it was, then the preventable deaths that it caused cannot be called unexpected (and this has serious ramifications for the people who made the decisions).
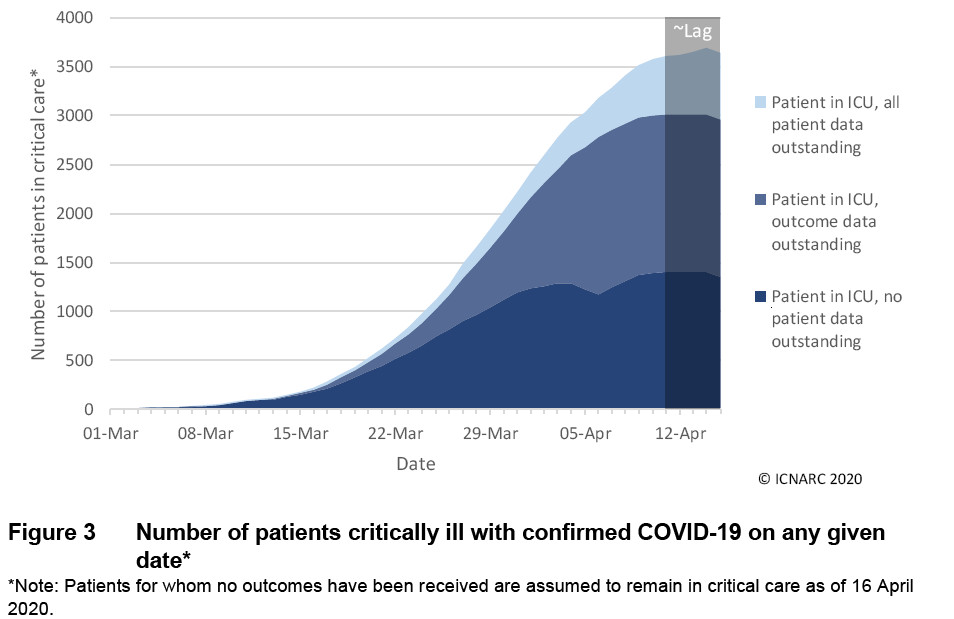
Moving on to the matter of “real” Covid-19, our more realistic indicator, which is the ICNARC audits, in their most recent manifestation (dated 17th April), show that the percentage change for critical care bed occupancy has declined again (so that the pattern that was first recorded in these pages, here, looks like this: 274%, 150%, 44% and 20%). 2642 patients were being treated in critical care at the time of the latest ICNARC audit.
In the body of this latest audit one can find a graph that indicates that the Easter peak of Covid-19, so much written of hereabouts, did indeed take place. In appreciating this graph, the reader should understand that ICNARC categorises patients according to the sort of notification it receives about them from the hospitals. First of all there are patients of whom ICNARC have received notification regarding admission. Then there are patients of whom ICNARC have received notification regarding first 24-hour physiology notification. This is the figure that FBEL uses because it is felt that this stage of notification serves as proper verification of a patient in critical care. ICNARC also receives notification of an outcome for each patient, and this involves either the patient having died, or having been discharged from intensive care. The graph contains no more data after 15th April, and the ICNARC audit appertains to information collated up to 4pm on the 16th. So, on the graph, we would expect to see the line for “Patient in ICU, outcome data outstanding” dip further as it travels beyond the limit of the x-axis.
Of course, there is another strata of trueness as far as Covid-19 is concerned, as was pointed out in a previous FBEL article (link above):
Let’s recap. Covid-19 is supposedly a pneumonia as a complication of SARS-COV-2, but we’ve found that:
For most people, “Covid-19” is a mild illness which is never confirmed as being due to SARS-COV-2, but the perception of its reality is created by official general prognosis.
A developed SARS-COV-2 infection could be flu, or even a bacterial infection, and “Covid-19”, or the pneumonia associated with it, would in fact arise as a complication due to these other causations.
Pneumonia or severe respiratory complications can occur from a treatment for cancer – which incriminates other pre-existing conditions in combination with their medical treatments…
Meanwhile, quite astonishingly, there is no acknowledgement of what might be true Covid-19, which is an infection of the lungs related to the interaction between SARS-COV/SARS-COV-2 and Angiotensin-Converting Enzyme 2 (ACE2) that is promoted in treatment by prescribed drugs.
When it boils down to it, Covid-19 could be a very specific illness, and the numbers presented by ICNARC could actually be precisely representative of that.
Now, usually the previous sentence would be followed up by the making of a case, again, for the ending of the lockdown – but this time, this is beyond our scope. The point on this occasion is to impress upon the reader the extent to which the UK Government’s reaction to Covid-19 has been way beyond anything anyone could call proportional. It has been unnecessarily, grotesquely exaggerated, and pointlessly damaging, and that’s why one should not accept the idea that is now emerging in the coronavirus zeitgeist created by corporate and social media that the UK Government has but made a mistake, and should be forgiven when it puts things right.
It should be increasingly obvious that UK Government has used the notion of protecting the NHS from something that shouldn’t have troubled it (any more than a usually bad flu season would have) for nefarious ends. The economic woes that will have been caused by the lockdown in the name of the NHS are to be diabolical; for example: “Britain’s economy could shrink by 35% this spring and unemployment soar by more than 2 million”.
Naturally, the democide committed at this time by UK Government has been appalling, but one mustn’t forget that, through the NHS as usual, it is a weekly, monthly and yearly reality, Covid-19 or no Covid-19. The new and unusual crime is the deliberate wrecking of the economy, and in perpetrating it, Government would have endangered the living and the livelihood of those who would not so fecklessly put themselves into the hands of NHS, or the greater welfare state, to become a victim in that respect. It is one thing when UK Government disposes of those who have already surrendered to it. It is another to go to war with those who will not surrender. This is why it has picked a fight too far. It won’t win.















Effectively treason has been committed and once the people of this country have thrown out Bill Gates and his deep state hoodlums we will make sure there are politicians who will face Jail time as well as media bosses who were in the deception to strip our economy and rights and begin one of the largest genocides the world has seen. Furthermore the Royal Family are done! No more evil bloodlines and greed capitalism… This things only just started.
Now factor in the ‘curative’ related deaths in ICNARC fogure (https://www.globalresearch.ca/are-ventilators-killing-more-people-than-saving/5709562) and a more sinister picture can be painted. Just as with the cause of death speculation clause that the Coronavirus Bill allows, there is also provisions for indemnity against malpractice for any coronavirus treatment. It indicates premeditated murder on the part of the state in order to boost the death rate. Combine this with the lack of testing/faulty tests and this can be understood further in the context of high fatality ratio which the government continues to use as justification for the repressive and profoundly destructive measures.